

Turner syndrome (TS) is named after an American endocrinologist Dr. Henry Turner in 1938, who described 7 women patients with short stature and absence of female sexual characteristics, increased skin folds in the neck and wide carrying angle of the arms.
The incidence is about 1 in 2000 live female births.
Those who are not treated for short stature during childhood will eventually be short adults (about 20 cm shorter than their normal expected height).
The good news is that when TS is diagnosed early (younger than 12 years old before the cessation of growth), growth hormone therapy can improve the final adult height.
Aetiology
TS is a chromosomal abnormality that modifies development in females.
Chromosomes carry human genes and the human species has 23 pairs, of which one pair is the sex chromosomes (XX in a girl or XY in a boy).
The sex chromosomes are important for fertility and sexual characteristics of a gender.
Girls with TS are born with only one X chromosome or incomplete/abnormal X chromosome. This occurs as a random error during formation of either the ovum or the sperm. (This is not related to poor maternal dietary habit or side effects of medication).
Clinical Features and Other Associated Problems
The physical manifestations vary widely among girls with TS. It depends on the proportion of the body’s cells that is affected by the abnormality in the X chromosome.
Some girls have many physical features of TS, whereas others may have only a few medical problems. Short stature can be the only physical feature in a very young girl.
The two main clinical features of TS are short stature and the lack of the development of the ovaries, which occur in almost all patients.
- Short Stature
They may have normal height in the first two years of life, after which a slow growth rate can usually be seen and worsen as they get older. During sexual maturation, they do not have the growth spurt as observed in normal girls and eventually growth into short adults. - Lack of Sexual Maturation
Almost all girls with TS have non-functioning ovaries and thus cannot produce sex hormones (estrogen and progesterone). Therefore, they do not develop breasts and do not have menses during adolescence. Though they have normal womb and vagina, almost all girls with TS will not be able to become pregnant without medical intervention. - Other Physical Abnormalities of Turner Syndrome:
- Loss of bony prominence of the 4th and 5th knuckles (refer picture 3)
- Increase carrying angle of the forearms (refer picture 5)
- Higher tendency to have moles on the skin
- Swelling or extra fluid in the hands and feet during newborn period (refer picture 2)
- Wide neck (webbed neck) and a low hairline at the back of the neck (refer picture 4)
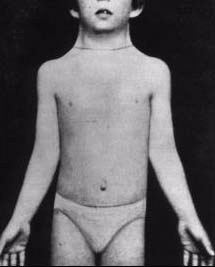
- Broad chest and widely spaced nipples (refer picture 5)
-
Other Associated Problems
- Intelligence: usually normal but may experience learning difficulties especially in mathematics, map reading, directions and visual organization.
- Heart anomalies: occur in about 20-30% of girls. Examples are narrowing of the aorta (a blood vessel from the heart), aortic valvular disease and aortic dissection. Risk for developing high blood pressure is also higher.
- Kidney anomalies: occur in about 25% of girls such as a horseshoe kidney.
- Ears: They may have frequent middle ear infections during early childhood and can sometimes lead to hearing impairment.
- Bones and joints: Osteoporosis or weakening of the bone occurs due to a lack of estrogen. This can be prevented to some extent by sex hormone replacement therapy. Other possible skeletal problems include scoliosis (curvature of the spine), congenital hip dysplasia.
- Higher risk of getting certain diseases: diabetes mellitus (especially in older and over-weight women with TS), celiac disease, hypothyroidism and hyperthyroidism.
- Eyes: minor problems (usually corrected by glasses), squint.
- Teeth: mild orthodontic anomalies
- Self-esteem: Because TS can affect how a girl looks and develop, some girls may have problems with body image or self-esteem.
Diagnosis and Investigations
TS is suspected when there is a number of characteristic physical features observed.
However, some Turner girls may not have obvious physical features and short stature can be the only physical manifestation during childhood. Some girls were detected during adolescents because of absent female sexual characteristics plus short stature.
This condition is sometimes recognized late in life when a patient demonstrates severe short stature, absent female sexual characteristics and infertility.
Occasionally, this condition is diagnosed during neonatal period when the newborn has characteristic left sided heart defect and oedematous/swollen hands and feet.
Confirmation is by a blood test, called chromosome test. The test counts the number of chromosomes and can identify any of the abnormally shaped or missing pieces. A result showing 45, X or other variants confirms TS.
If the chromosome test reveals that a girl has TS, her doctor may request additional tests to check for other problems that are often associated with TS.
Rarely, TS is suspected before a child is born, through an ultrasound test. This can be confirmed by prenatal testing – chorionic villous sampling or amniocentesis – to obtain cells from the unborn baby for chromosomal analysis.
Treatment
With early and appropriate medical care and ongoing support, most people with TS can lead normal and healthy lives.
Growth Hormone Therapy
Growth hormone therapy has been shown to improve final adult height in girls with TS, 141 cm vs 148 cm in untreated and treated girls.
Early suspicion of TS and referral to a Paediatric Endocrinologist before the age of 12 years enables optimization of final adult height with growth hormone therapy. Growth hormone therapy (daily subcutaneous injection) should be considered as soon as growth failure is demonstrated.
Sex Hormone Therapy
Girls with TS needs sex hormone therapy to develop physical changes of puberty, including breast development and menstrual periods besides preventing osteoporosis.
Sex hormones therapy (oral estrogen) can be started after the age of 12 years (or later if patient is on growth hormone therapy in order to optimize growth potential). Oral progesterone is added later for monthly ‘period,’ and to keep the womb healthy. Lifelong sex hormone replacement is needed.
Management of Other Associated Anomalies
- Those with abnormal heart may need surgical procedure to correct the problem.
- Patients with recurrent middle ear infections, which may lead to hearing impairment, need medical treatment and monitoring.
- Almost all women with TS are infertile. Pregnancy with donor embryos through in vitro fertilization technique has been reported. Proper supportive cares needed for the woman to carry the pregnancy to term.
- Regular health checks are very important for early preventive care.
- Due to higher risk of osteoporosis, patients must ensure adequate intake of calcium and vitamin D. Supplementation should be considered, especially from age 10 years onwards.
- Blood pressure should be checked routinely.
- They should also be monitored for thyroid diseases and diabetes mellitus during routine health checks
Having appropriate medical treatment and support allows a woman with TS to lead a normal, healthy and happy life.
Tips for Parents:
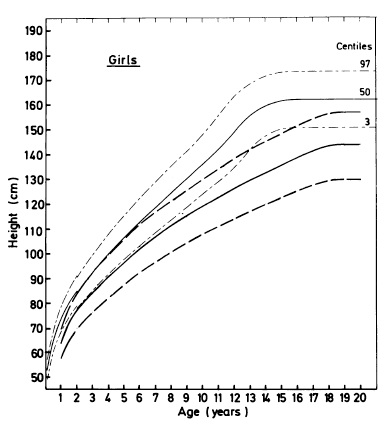
Short stature may be the only clinical feature of a very young girl with TS. Therefore, suspect TS if a girl exhibits poor growth (eg. shortest in class, and/or growth velocity < 5 cm per year) during childhood years. (Refer picture 1).
 |
|
Pictures 1: Growth Chart for Turner Syndrome Girls (Mean height (2 SD) at different ages on patients with Turner syndrome (heavy lines) plotted on a growth chart for normal girls (faint lines).
|
 |
 |
|
|
Picture 2: A Turner syndrome girl with swollen feet during neonatal period.
|
Picture 3: Loss of bony prominence of the 4th and 5th knuckles.
|
|
 |
 |
|
|
Picture 4: Wide neck and low posterior hairline in a girl with Turner syndrome.
|
Picture 5: Increase carrying angle of the forearms, wide neck (webbed neck), broad chest and widely spaced nipples in a girl with Turner syndrome.
|
|
Reference:
- Growth curve for girls with Turner syndrome. A J Lyon, M A Preece, D B Grant. Archives of Disease in Childhood, 1985, 60: 932-935.
- 2. Prevalence of cardiovascular malformations and association with karyotypes in Turner’s syndrome. Gotzsche CO, Krag-Olsen B, Nielsen J, Sorensen KE, Kristensen BO. Arch Dis Child. 1994;71(5):433.
- Prevalence of renal malformation in Turner syndrome. Flynn MT, Ekstrom L, De Arce M, Costigan C, Hoey HM, Pediatr Nephrol. 1996;10(4):498.
- Turner Syndrome: Diagnosis and Management. Thomas Morgan. American Family Physician, 2007, 76(3): 405-410.
- The Use of Growth Hormone in Children and Adults, Clinical Practice Guidelines, MOH/P/PAK/213.10(GU)
| Last Reviewed | : | 28 August 2020 |
| Translator | : | Dr. Janet Hong Yeow Hua |
| Reviewer | : | Dr. Zainab bt. Kusiar |





