

Ambiguous genitalia, also called the disorder of sex development, is a condition when a child’s external sex organs are not clearly male or female. The infant may appear different than expected.
The parents of infants who have ambiguous genitalia can get help from the healthcare team to assist them decide what is best for their children. Always remember that you are not alone. Work closely with your health care team.
Signs and Symptoms
A child’s sex can normally be determined at birth by the appearance of the external genitalia. However, this may not be obvious in some children because the child’s genitals did not develop properly.
There are various causes of ambiguous genitalia. One of the causes is congenital adrenal hyperplasia (CAH). It is important to rule out CAH in any newborn with ambiguous genitalia because an undiagnosed infant may encounter a life-threatening event during early infancy period (between 1 week to 3 months of age).
Infants with classical CAH have ambiguous genitalia, dark/pigmented skin/lips/nipples/nail beds (Picture 1), feeding intolerance and poor weight gain. They have excess male hormones (testosterone) and lack hormones like cortisol and aldosterone, which is needed to maintain water and electrolyte (sodium and potassium) balance. Without treatment with appropriate hormones, these patients may die of salt wasting and dehydration during early infancy.
Aetiology
Before a child is born, many steps must occur during development in the mother’s womb to determine a baby’s sex. The father and mother’s DNA combine to form a male or female embyo. A female embyo will have 46,XX as the genetic component while a male embyo will have 46,XY.
Each embryo starts out with 2 gonads and no sexual organ yet at this early stage. The gonads eventually develop into ovaries in a female and testes in a male (genetic abnormities can cause abnormal gonadal development).
Then, other reproductive organ such as uterus in females starts to form. The testes in males will gradually descend from the abdomen to the scrotum.
The external genitalia, ie the vagina or penis, begin to form around 6 weeks of life in the mother’s womb.
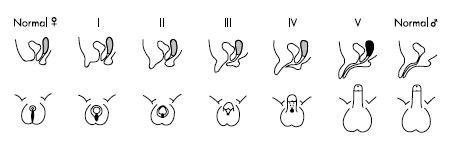
Genetic or hormonal defects can result in various abnormalities of the external genitalia (Picture 2).
It is important to understand that parents did not do anything wrong during pregnancy to cause ambiguous genitalia in their child. Certain factors (genetic, hormonal or other unknown factors) have disrupted the normal development of the child’s sex organs while in the womb.
Investigations
It is of utmost importace to assign the most appropriate gender before your child is named and thus the routine birth registration must be delayed.
A letter from the health care team will be issued to the birth registration department to explain the delay.
To decide the most appropriate sex assignment for the child, various factors must be taken into consideration, which include medical, social and to some extent religious factors.
Various tests are done in a specialized medical center to have a better understanding about the child’s sex development while in the womb. Tests may include the following:
- Chromosome study to determine whether the genetic make up of the child is 46,XX or 46,XY.
- Ultrasound to visualize the internal sex organs (uterus or intra-abdominal gonads). Please note that the uterus in a newborn baby may not be easily visualized and therefore the inability to visualize it by ultrasonography does not necessarily indicate absence of uterus.
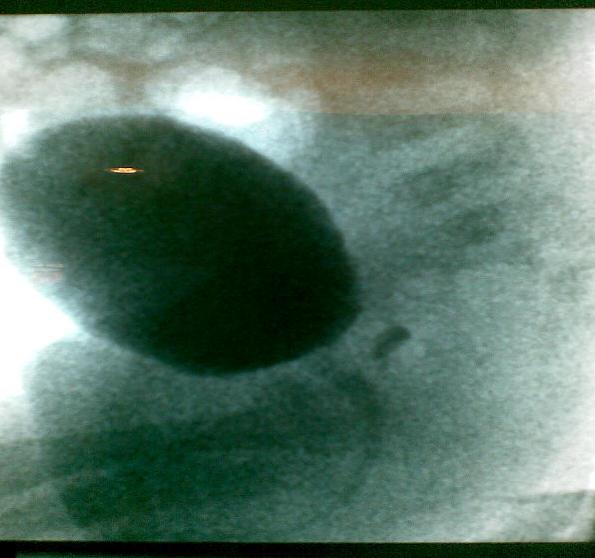
- Genitogram to help identify the internal sex organ (eg. uterus), and to delineate the genital tracts (vagina and urethra) (Picture 3). This procedure involves the insertion of a soft catheter (urinary catheter) through the urethra for introduction of a special dye into the genital tracts, followed by radiography.
- Biochemical tests and various hormonal tests to understand the hormonal status of the child.
Complication
The decision-making is extremely difficult for both doctors and parents when a child is born with ambiguous genitalia. Everyone involved wants to make the best decision for the child. The best decision will be the one which proves to be right in the long term and which corresponds most closely to the individual’s deepest sense of self as an adult.
However, faced with parents’ strong emotions, it may be tempting to operate away the problem soon after birth. Parents should be aware that they might face bitter resentment if their grown-up children are not content with their surgery or their assigned role. Therefore, parents should not have the impression that one quick operation will put things right forever. They must work closely with the health care team.
Tips for Parents:
- It is important to discuss openly with the health care team and any doubt or concern raised be clarified with them.
- It is important to be patient regarding the sex assignment in your child. Do not rush into making decision without proper investigations by the health care team. Work closely with your health care team to understand the various factors influencing a child’s gender, which is not determined just by the appearance of the external genitalia. Learn more about your baby so that you can decide the best sex in which to raise your child. This will help your child to live a happy and normal life.
Treatment
The health care team include some or all of these members:
Paediatric Endocrinologist: A doctor who specializes in diagnosing and managing conditions related to hormones, is the key member in the team.
Pediatric surgeon specializes in genital surgery: A doctor who specializes in surgery of the female and male genital tracts in children.
Psychologist: A specialist who helps your child and family cope with emotional stress encountered while dealing with your child’s condition.
Social worker: A dedicated trained person to help you cope with social and financial issues arising from your child’s condition
Genetic specialist: A specialist who can help determine whether what caused your child’s condition is genetic (runs in your family). This will help you understand whether your future pregnancy is more likely to be affected by ambiguous genitalia.
Treatment depends on the type of disorder a child has. Some conditions are treated with surgery, which may involve reconstructing external genitalia or removing internal sex organ.
In some cases, more than one surgery is needed. Sex hormones to induce secondary sexual characteristics in males and females may be needed in some children around the age of 12 years.
Lifelong sex hormone replacement may be needed in those with hypogonadism (no functional testes or ovary).
Oral medications such as hydrocortisone and fludrocortisone must be started timely for patients with ambiguous genitalia due to CAH.
When should surgery be done?
If surgery is needed, your child’s healthcare team will discuss with you when is the best time to operate. In some cases, it is recommended to wait until adolescence. This is to allow your child more time to grow.
Supporting Organizations
Keep in mind the following::
- You are not alone. Members of your child’s healthcare team will help guide you.
- Treatment is available. Counseling, medication, and surgery can help your child live a normal life.
- There are things you can do to help your child get a good start. Ask your child’s healthcare team for suggestions.
It is normal for parents to be emotional at the start. You may be worried thinking about your baby’s future. You may feel pressured to decide the sex of your child right away.
Remember that you have time to make this decision. Most importantly, remember that your child needs to be accepted, loved, and comforted. Learn to accept your child as he/she is and that no human beings are perfect. You should also get support for yourself.
Counselors/psychologists are available to help and support you in time of stress.
 |
 |
|
Picture 1: Ambiguous genitalia and hyperpigmented nail-beds in an infant with congenital adrenal hyperplasia |
|
 |
|
|
Picture 2. Differential virilisation/masculinization of the external genitalia using the staging system of Prader, from normal female (left) to normal male (right). Side view (upper panel) and horizontal cross sectional (lower panel) views shown. |
|
|
|
|
| Picture 3: Genitogram showing urinary bladder and urogenital sinus | |
| Last Reviewed | : | 28 August 2020 |
| Writer | : | Dr. Janet Hong Yeow Hua |
| Reviewer | : | Dr. Zainab bt. Kusiar |





