

Introduction
DiGeorge Syndrome also known as 22q11.2 deletion syndrome is a disorder caused by the deletion of a small region of chromosome 22. The deletion occurs at q arm (long arm) on chromosome 22 at location q11.2.
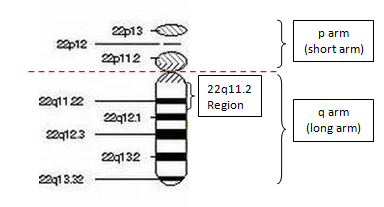
Figure 1: Chromosome 22
There are many symptoms that reflect DiGeorge Syndrome. It can affect almost any part of the body. Even among affected members of the same family, the features of this syndrome vary. Common clinical features of DiGeorge Syndrome includes congenital heart defect (abnormality in the heart that are present at birth), cleft palate (an opening in the roof of the mouth) and distinguish facial features.
Children with DiGeorge Syndrome possess common features such as growth and speech developmental delays (i.e. sitting up, rolling over, walking) and learning disabilities. At a later stage of life, they also have a chance of developing mental illness such as depression, anxiety, bipolar disorder and schizophrenia. Furthermore, in comparison with normal children, DiGeorge Syndrome’s patients are prone to have attention deficit hyperactivity disorder (ADHD), developmental conditions such as autism spectrum disorders that affect communication and social interaction.
Earlier on, medical practitioners describe patients with DiGeorge Syndrome as different disorders because this syndrome reflects vary features. They were named as Velocardiofacial Syndrome (also known as Shprintzen Syndrome), and Conotruncal Anomaly Face Syndrome. Moreover, there are cases whereby individual with this deletion was diagnosed with the autosomal dominant form of Opitz G/BBB Syndrome and Cayler Cardiofacial Syndrome. After the genetic origin for all these disorders was known, medical practitioners concluded that they were all part of one syndrome with many possible symptoms and features (DiGeorge Syndrome). To further elude misunderstanding, a description based on its genetic origin, this condition (with many signs and symptoms) is usually called DiGeorge Syndrome or 22q11.2 deletion syndrome.
Prevalence
DiGeorge Syndrome affects an estimated 1 in 2000 to 4000 livebirth with 5 to 8 percent child having cleft palate. However, the disorder may actually be more common than reported. The wide variation of features in DiGeorge Syndrome may have caused it to be under diagnosed (due to mild symptoms) or misdiagnosed with other disorders (overlapping features).
Other Related Health Issues
Individuals with DiGeorge Syndrome will frequently have recurrent infections caused by problems with their immune system. Some even develop an autoimmune disorder in which the immune system attacks the body’s own tissues and organs. Affected individuals may also have;
- Breathing problems
- Kidney abnormalities
- Low calcium level in the blood (which can result in seizures)
- Decrease in blood platelets
- Feeding difficulties
- Gastrointestinal problems
- Loss of hearing
- Wound that won’t heal properly
- Immune system problem
Identification & Screening
It is difficult to diagnose DiGeorge Syndrome due to the fact that the condition affects each child differently, it can display different symptoms that often vary in severity, and can be associated with many other disorders.
If a child is suspected to have a chromosome 22q11.2 deletion, medical practitioners will probably refer them for genetic testing to confirm the diagnosis such as Cytogenetics Tests and Fluorescence in situ hybridization (FISH).
A thorough medical examination and a gathering of family history will be carried out by clinician before suggesting for genetic testing.
A cytogenetic test is a conventional genetic testing that looks at the changes in number and structure of the chromosomes (chromosome are the structure in the nucleus of the cell that carries DNA).
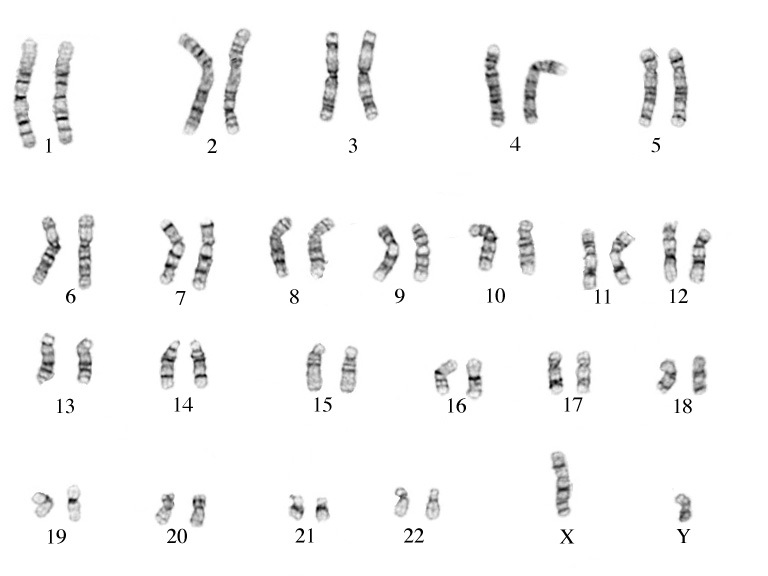
Figure 2: A normal male karyotype (46,XY) by conventional cytogenetics.
FISH test is a molecular cytogenetics technique that detects deletion of a specific sequence on a chromosome using a complimentary fluorescence probe that binds to the targeted DNA sequence.
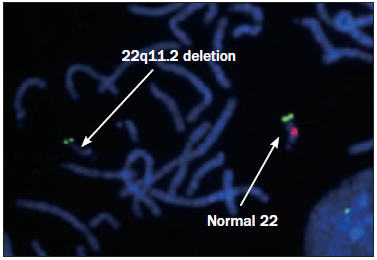
Figure 3: Deletion in the DiGeorge Syndrome critical region on chromosome 22 detected by FISH test.
Cure & Treatment
A genetic condition such as DiGeorge Syndrome cannot be cure. However, various treatments could be given to affected child depending on the child’s symptoms. Affected children with DiGeorge Syndrome will be recommended to undergo evaluation in the areas where medical practitioners know the chromosomal deletion can affects and it will help the child to live through life as healthy as possible.
A DiGeorge Syndrome child may require an evaluation and treatment in the following areas: cardiology (heart), child development and psychology, cleft palate (plastic surgery could correct the anomaly), ENT and audiology, endocrinology, immunology, urology, neurology and genetics. It is important to take an affected child to a yearly evaluation with a geneticist as geneticist knows the latest update with the research done on any genetic condition and also they can answer questions about the affected child’s general care.
References
- http://ghr.nlm.nih.gov/
- http://www.chop.edu/conditions-diseases/chromosome-22q112-deletion
- http://www.mayomedicallaboratories.com/
- http://worms.zoology.wisc.edu/
| Last Reviewed | : | 07 April 2017 |
| Writer | : | Nur Ashikin Azemi |
| Accreditor | : | Farah Amalina bt. Mohd Zulkufli |





