

Introduction
Impacted teeth defined as retained teeth in the jaw beyond their normal date of eruption. An impacted tooth which remains in the jaw for various reasons. The tooth becomes impacted because eruption is interrupted or obstructed by adjacent teeth, dense overlying bone or excessive soft tissue, malpositioning or lack of space in the arch. These impacted teeth may, therefore, be non-functional, abnormal, or pathological.
Impacted tooth can be partially erupted or completely unerupted. Partially erupted means the tooth is seen in the mouth but failed to erupt into a normal position and is unlikely to erupt completely. Whereas completely impacted means the tooth is totally embedded and covered by soft tissue and bone, therefore it is unable to erupt.
The most common impacted teeth are the third molars, followed by maxillary canines and mandibular premolars.
Third molars are the most frequently impacted because they are the last tooth to erupt and most likely to have inadequate space to erupt. In the mandible, the most common location of such third molars is in the ascending ramus. In the maxilla, the teeth can displace as far as to the floor of the orbit. Impacted third molar is one of the common findings which detected during a routine dental checkup. However, the patient usually seeks treatment whenever there are clinical symptoms.
Upper canines (in the maxilla) are the second most frequently impacted teeth after the third molars. The incidence of impaction for an upper canine is 20 times higher as compared with lower canine impaction (in the mandible). Almost 50% of the upper canine is palatally impaction, 30% with buccal impaction and followed by 20% in the intermediate position (impaction occur between palate and buccal bone).
Usually, in the anterior maxilla, the canine tooth prevented from erupting due to crowding from the other teeth. The maxillary canine will erupt after the eruption of maxillary lateral incisor and first premolar. Thus it becomes impacted should space is inadequate, therefore unavailable to allow eruption.
Impaction of the lower (mandibular) canine is not common. In some situations, the tooth bud of the lower canine happens to rotate in the basal bone of the mandible. For that reason, the canine root can develop in a horizontal direction and becomes impacted below the apices of the incisors.
The prevalence of impacted premolars seems to vary according to age. The lower (mandible) second premolars rank third after third permanent molars and maxillary canines. If the first molar and canine tooth to erupt earlier than premolar, therefore the premolar will become impacted as a result of limited space for tooth eruption.
Impaction of incisors usually encountered when the child’s age between 8-10 years. Impaction of upper (maxillary) central incisor occurs commonly due to the presence of supernumerary or mesiodens. Impaction of lower (mandibular) incisor is very rare and usually associated with cysts.
Types Of Impaction
The diagrams below show types of impaction for commonly impacted teeth.
- Impacted Maxillary Third Molar
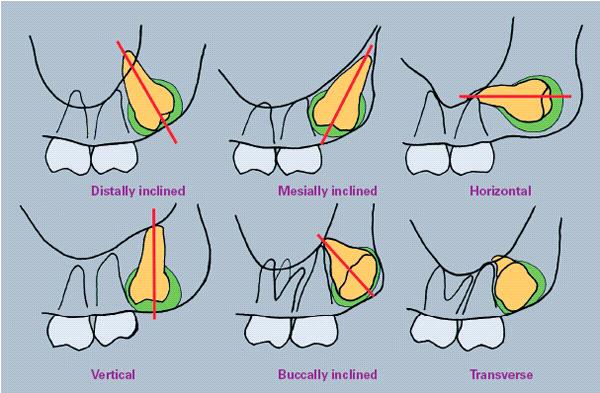
Source: www.pocketdentistry.com - Impacted Mandibular Third Molar
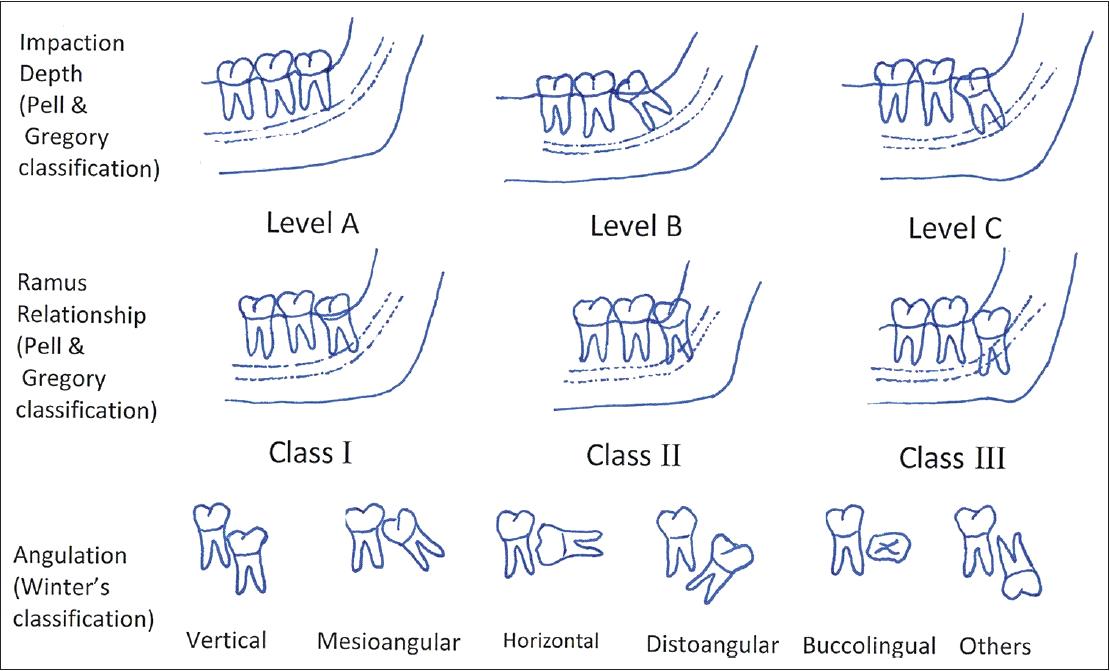
Source: M Eshghpour et al. Pattern of mandibular third molar impaction: A cross-sectional study in the northeast of Iran. Niger J Clin Pract. 2014;17(6): 673-677. - Impacted Maxillary Canine
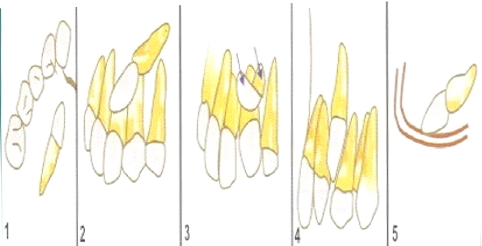
Source: http://www.slideshare.net/koli_tanvi/impaction- Palatally placed
- Labially placed
- Partly on the labial side and partly on palatal side
- Canine locked between the roots of adjacent teeth
- Canine in the edentulous maxilla
Aetiology Of Tooth Impaction
- Local Factors
- Lack of space due to the imperfect development of the jaws.
- Obstructions of the soft or hard tissue by retained deciduous teeth, odontome, cysts or odontogenic tumour.
- Abnormal path of eruption of the tooth due to traumatic forces during eruption period.
- Irregularity in the position and pressure of an adjacent tooth.
- Systemic
- Prenatal
- Hereditary
- Prenatal
- Postnatal
- Rickets
- Congenital Syphilis
- Tuberculosis
- Malnutritions
- Endocrines diseases
Indications For Removal Of Impacted Teeth
- Infections such as pericoronitis, abscess, cellulitis
- Unrestorable caries or prevention
- Periodontal diseases or prevention
- Associated with pathology
- Orthodontic reason
- Prior orthognathic surgery
- Prophylactic removal in the presence of medical and surgical conditions
- Tooth in a fracture line
- Pain of unknown origin
Contraindications For Removal Of Impacted Teeth
- Presence of adequate space for the eruption of impacted teeth
- Patients with no history of any bony pathology
- Patients whose medical history renders the removal of teeth or when the risks exceed the benefit.
- Partially impacted teeth which can be used as an abutment in the construction of fixed partial denture.
Radiographic Assessment
- Radiographic assessment is done to assess:
- Orientation (e.g.,. mesioangular, vertical, distoangular, palatal or buccal )
- Depth below the occlusal plane
- Crown size and follicular width
- Root morphology (number, length, shape: fused or separate, curved apex, bulbous, ankylosis).
- Condition of the crown and the adjacent tooth
- Approximation of an ascending ramus, Inferior Dental Canal, maxillary sinus, pterygoid plates and pyriform fossa.
- Radiographic assessment
- Intraoral view: periapical and occlusal views
- Extraoral view: OPG, lateral skull and CBCT.
Treatments Available For Impacted Teeth
Treatment options:
- No treatment
- Conservative management
- Surgical repositioning and transplantation
- Exposure of the teeth with or without orthodontic application
- Surgical removal
As a general rule, teeth should not be removed without an appropriate indication.
References
- James R. Hupp, Myron R. Tucker, Edward Ellis III, Contemporary Oral and Maxillofacial Surgery, 6th edition, Mosby, 2013.
- SM Balaji, Text book of Oral and Maxillofacial Surgery, Elsevier, 2009.
- M Eshghpour et al. Pattern of mandibular third molar impaction: A cross-sectional study in the northeast of Iran Niger J Clin Pract. 2014:17(6): 673-677.
- http://www.pocketdentistry.com
- http://www.slideshare.net/koli_tanvi/impaction
- http://jasonerasmus.com/procedures/impacted-canines
| Last Reviewed | : | 06 March 2017 |
| Writer | : | Dr. Sundrarajan Naidu a/l Ramasamy |
| Accreditor | : | Dr. Khairulzaman bin Adnan |





