

Introduction Of Spinal Cord Injury (SCI)
Definition:
Spinal cord injury occurs when there is any damage to the spinal cord that blocks communication between the brain and the body. After a spinal cord injury, a person’s sensory, motor and reflex messages are affected and may not be able to get past the damage in the spinal cord. In general, the higher on the spinal cord the injury occurs, the more dysfunction the person will experience. Injuries are referred to as complete or incomplete, based on whether any movement and sensation occurs at or below the level of injury. Each person’s recovery from spinal cord injury is different.
Causes:
- Traumatic Injuries such as motor vehicle accidents, fall, acts of violence, sports and recreational injuries.
- Non Traumatic injuries/ illness such as Cancer, Arthritis, Multiple Sclerosis, Osteoporosis and Inflammation of the Spinal Cord.
Risk Factor:
Spinal cord injuries affect more men than women. The majority of people who sustain a spinal cord injury are young adults between the ages of 16 and 30 because of riskier behaviors.
Symptoms:
Your ability to control your limbs after spinal cord injury depends on two factors:
- The location of the injury along your spinal cord and
- The severity of injury to the spinal cord.
The lowest part of your spinal cord that functions normally after injury is referred to as the neurological level of your injury. The severity of the injury is often called “the completeness” and is classified as either of the following:
- Complete Injury: The injury is completeif almost all feeling (sensory function) and all ability to control movement (motor function) are lost below the level of traumatic lesion.
- Incomplete injury: The injury is incomplete if there is some preservation of motor or sensory function below the level of injury including the sacral segments. There are varying degrees of incomplete injury.
Additionally, paralysis from a spinal cord injury may be referred to as:
a) Tetraplegia
- Due to lesion at or above T1.
- Damage to the spinal cord in the neck area (cervical segment) can result in complete or partial paralysis of the arms, hands, trunk and pelvic organs.
- Breathing is only affected by injuries high on the spinal cord. But bowel and bladder control can be affected no matter where the spinal cord is injured.
b) Paraplegia
- Due to lesion below T1.
- Damage to the spinal cord at T1 and below can result in complete or partial paralysis of the lower body, legs and pelvic organs.
Signs and Symptoms:
Spinal cord injuries of any kind may result in one or more of the following signs and symptoms:
- Loss of movement
- Loss of sensation
- Loss of bowel or bladder control
- Exaggerated reflex activities or spasms
- Changes in sexual function, sexual sensitivity and fertility
- Pain or an intense stinging sensation
- Difficulty breathing, coughing or clearing secretions from your lungs
Spinal Cord Injury (SCI) Levels
Anatomy:
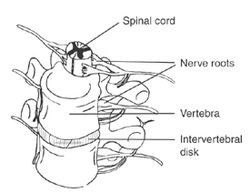
The spinal cord is divided into 31 segments, each with a pair of anterior (motor) and dorsal (sensory) spinal nerve roots.
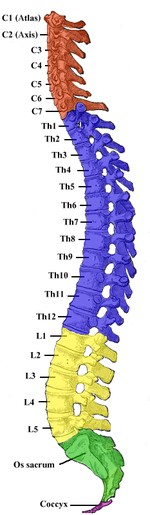
The spinal cord is surrounded by protective rings of bone called vertebrae. The vertebrae and spinal nerves are organized into segments , starting at the top of the spinal cord. Within each segment, the vertebrae and nerves are numbered. The segments are as follows:
- The neck area contains 7 cervical vertebrae (C1 through C7) and 8 cervical nerves.
- The chest area contains 12 thoracic vertebrae (T1 through T12) and 12 thoracic nerves (T1 through T12).
- The lumbar area (between the chest area and the pelvis) contains 5 lumbar vertebrae (L1 through L5) and 5 lumbar nerves (L1 through L5).
- The sacral area (from the pelvis to the end of the spine) contains 5 sacral vertebrae (S1 through S5) and 5 sacral nerves (S1 through S5).
 |
 |
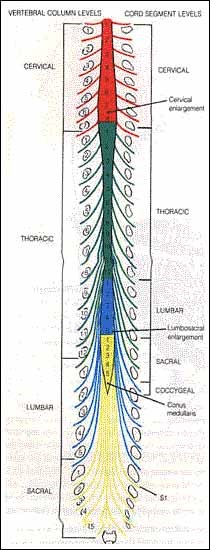 |
| View of the vertebral column and spinal cord | Spinal Vertebrae |
Spinal Cord |
Types Of Wheelchair & Criteria To Choose The Wheelchair
Type of wheelchairs
- Manual Wheelchair
- Power Wheelchair
Type of Manual Wheelchairs:
- Standard wheelchair
- Light weight wheelchair
- Reclining wheelchair
- Children wheelchair
- Sport wheelchair
- Racing wheelchair
 |
 |
| Manual Wheelchair | Power Wheelchair |
Type of Power wheelchairs:
- Hand Control
- Chin Control
- Head Control
- Breath control
How Can Physiotherapy Help In Wheelchair Skill?
Since most SCI patients use wheelchairs as their sole method of locomotion, they should be equipped with a wheelchair that fits and is adjusted properly as soon as they begin out-of bed activities.
Following are the skill prerequisites for:
- doing pressure reliefs in a wheelchair
- propelling wheelchairs over even terrains,
- Transferring without equipment set up
- Self-transfer from wheelchair to toilet seat
- Propelling wheelchair over obstacles: Ramp & wheelchair terrains
- Wheelie Skill
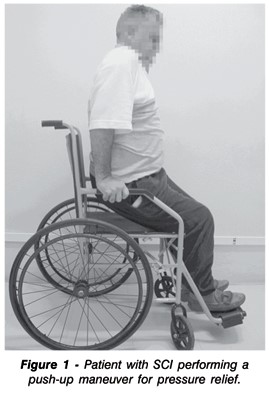
A. Doing Pressure Relief in a Wheelchair
The single most important functional skill required by all SCI patients is the ability to perform pressure reliefs to prevent pressure sores, from developing on the buttocks and on the skin over the ischial tuberosities and other boney prominences during sitting.
Functional Skills – Pressure relief should be performed every 15-20 minutes, in the beginning until skin tolerance improves.
- Pushup – The patient with adequate strength in the triceps places the hands lateral to the buttocks on the wheelchair seat, armrests, or wheels, extends the elbows, depresses the shoulders, and pushes down to raise the body.
 |
 |
 |
Push Up Weight Shift: Side Lean
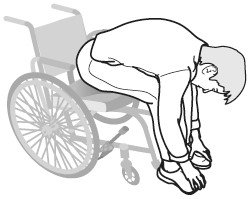
2. Weight Shift – The patient leans far enough forward to unweight the ischial tuberosities, or, leans to one side, and then the other side, to unweight one side at a time.
B. Propelling Wheelchairs over Even Terrains/Surfaces
- Functional Skills
- With Finger Flexors – The patient grasps the hand rims and pulls forward or backward to move the wheelchair.
- With Finger Flexors – The patient grasps the hand rims and pulls forward or backward to move the wheelchair.
 |
C. Transferring Without Equipment Set up:
-
- Position the wheelchair at a 45? angle to the surface to be transferred. Remove both leg rests, remove the arm rest that is in the direction of the transfer.
- Move buttocks forward on the sitting surface
- Position hands in front of the trunk – one hand on the sitting surface or arm rest of the wheelchair, the Other hand on the seat of the destination of the transfer
- The individual then locks the elbows using muscle substitution or supports his/her body weight using the triceps
- Lean forward onto both upper extremities and tuck the chin downward
- The individual then quickly and forcefully moves his/her head and shoulders down and away from the destination of the transfer – thus lifting your buttocks up and moving it towards the.
D. Self-Transfer From My Wheelchair to the Toilet
- Move the footrests out of the way and move the wheelchair close to the front of the toilet.
- Put your feet flat on the ground in front of you. Lock the wheelchair.
- Move to the edge of your wheelchair. Slide your pants and underwear down to your ankles. Remove the clothes from one ankle so that you can spread your legs apart.
- Put your feet flat on the floor next to the sides of the toilet. Spread your knees and ankles wider than the toilet.
- Grab the safety bars next to and behind the toilet. Facing the wall behind the toilet, lift yourself up.
- Hold the safety bars, turn your body around, and lower yourself onto the toilet.
- After you have finished and transferred yourself back to your wheelchair, move the arm and footrests back into place.
E. Propelling Wheelchairs Over Obstacles: Ramp And Uneven Terrains
- Functional Skills
- Ascending – The functional skills to propel forward in Manual Wheelchair Propulsion are modified to add a forward lean of the head and trunk (where possible), to avoid jerking the wheels abruptly (to prevent tipping the chair), and to use shorter strokes and move the hands rapidly between pushes (to avoid rolling backward between pushes)
- Descending on 4 Wheels – The patient controls the chair, rather than propels it, when descending a ramp, by gripping the hand rims loosely, but with enough resistance to slow and control the chair’s descent, and allowing the hand rims to slide through the hands, or.
 |
 |
| Curb | Wheelie skill |
F. Wheelie Skill
A “wheelie” is the act of balancing on your rear wheels in your wheelchair. Wheelies may look like tricks, but “they are the essential building blocks of community wheelchair skills.
Why is Wheelie skill important?
- Improved quality of life
Several studies have shown that learning wheelies and related skills can improve your quality of life because they help you be more independent and more active in the community, such as going to school, work and social activities - Less pain, fewer falls
Overall, the purpose and important of learning wheelchair skill are as such:
- To improve his/her ability to safely and effectively use a wheelchair
- The purpose of these activities is to overcome barriers in the environment and to thereby permit the wheelchair user to fulfill his/her desired role in society.
- Other potential benefits of wheelchair-skills training for wheelchair users and caregivers include fewer acute and overuse injuries, improved sense of well being (through self-esteem, self-efficacy, confidence and personal control), improved development (of children) and having fun.
- Improve quality of life.
For further detail please refer to the link below:
- Wheelchair Skills Training Program(http://www.wheelchairskillsprogram.ca). by Dalhousie University (Canada).
- Wheelchair skills program (wsp) version 4.1 wheelchair skills training program (wstp) manual
Reference:
- Wheelchair Skills Training Program. Dalhousie University. Available at:http://www.wheelchairskillsprogram.ca/. Accessed September 18. 2010.
- Wheelchair skills program (wsp) version 4.1 wheelchair skills training program (wstp) manual
- Anneken V, Hanssen-Doose A, Hirschfeld S, Scheuer T, Thietje R. Influence of physical exercise on quality of life in individuals with spinal cord injury. Spinal Cord. 2010;48:319-399.
- Kilkens O, Post M, Dallmeijer A, van Asbeck F, van der Woude L. Relationship between manual wheelchair skill performance and participation of persons with spinal cord injuries 1 year after discharge from inpatient rehabilitation. J Rehabil Res Dev. 2005;42:65-74.
- The PoinTIS SCI Physical Therapy site of the SCI Manual for Providers is based on information in Spinal Cord Injury: Functional Rehabilitation, by M.F. Somers, Norwalk, CT, Appleton & Lange, 1992, and information in “Respiratory Rehabilitation of the Patient with a Spinal Cord Injury”, by J.L. Wetzel, B.R. Lunsford, M.J. Peterson, and S.E. Alvarez, Chapter 28 in Cardiopulmonary Physical Therapy, S. Irwin and J.S. Tecklin, eds., St. Louis, Mosby, 1995, unless otherwise indicated.
| Last Reviewed | : | 23 August 2019 |
| Writer / Translator | : | Wong Mui Fung |
| Accreditor | : | Haironi binti Ismail |
| Reviewer | : | Halimah bt. Hashim |





