

Oral tumour is a mass of abnormal tissue which arises from oral tissue with no obvious causes which stimulated the growth. It is characterized by independent and unrestrainable growth.
The disease can be categorized into two types; benign and malignant. The term “benign” implies for mild and non aggressive behavior . Some growth being called benign because of lack ability to invade surrounding structure and metastasis, but it may produced negative health effect on patient . The example of common benign tumour originate from oral and maxillofacial region are ameloblastoma, odontogenic cyst (e.g: dentigerus cyst , odontogenic keratosis ), central giant cell granuloma, fibrous osseous lesion and adenomatoid odontogenic tumour.
The etiology or causes of the tumour is unclear and most of diseases detected once the swelling already established. Occasionally, the disease might be detected by incidental finding during performing other investigations like x ray or routine clinical check up. The tumour usually slow growing, painless and pushing the surrounding structures.
These kind of tumour may cause facial deformity, jaws discrepancies, airway obstructions, reduced functional ability likes chewing , swallowing and eating.

Ameloblastoma of lower jaw
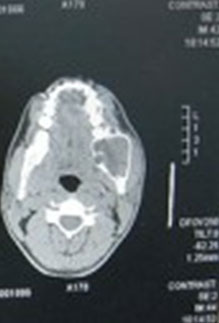
CT Scan shows tumour of left lower jaw

OPG x ray shows tumour of right lower jaw

Tumour has been resected
Management of tumour depends on the degree of disease. It is involved from simple surgery enucleation (dragging ), marsupiliasation( Decompression ) to major surgery likes resection and reconstructions with free flaps such as fibula graft or iliac bone.
The malignant type is a condition to become aggressive and potentially can cause death. Oral cancer is one of the most prevalence cancers, listed among the sixth commonest cancer worldwide and third commonest cancer in south east asia region where bête quid chewing is a common habit among ora cacer patient. More than 100,000 new cases detected every year in those area ( WHO 1984 ). In Malaysia , apparently, the overall prevalence was reported as 0.04% ( Zain et al 1997 ). Oral cancer was the five most commonest cancer in Peninsular after breast , colorectal, lung , cervix and nasopharynx ( Jatin P. Shah et a 2003 ). It is a subtype of head and neck cancer, that easily detected with oral examination. The cancerous tissue growth located in the oral cavity and It may arise as a primary lesion originating in any of the oral tissues or by metastasis from a distant site of origin, or by extension from a neighboring anatomic structure, such as the.nasal cavity.
Alternatively, the oral cancers may originate in any of the tissues of the mouth, and may be of varied in histological types: teratoma, adenocarcinoma derived from a major or minor salivary gland, lymphoma from tonsillar area or other lymphoid tissue, or melanoma from the pigment-producing cells of the oral mucosa. There are several types of oral cancers, but the most common is around 90% are squamous cell carcinomas, originating in the tissues that line the mouth and lips. Oral or mouth cancer most commonly involves the tongue. It may also occur on the floor of mouth, cheek lining, gingiva (gums), lips, or palate (roof of the mouth). Most oral cancers look very similar under the microscope and are called squamous cell carcinoma ( SCC ).
The exact cause of oral cancer is unknown, but it is important to note that around 75 percent of oral cancers are linked to modifiable behaviors such as tobacco use and excessive alcohol consumption. Other factors include poor oral hygiene, irritation caused by ill-fitting dentures and other rough surfaces on the teeth, poor nutrition, and some chronic infections caused by bacteria or viruses.
Betel nuts chewing is a common habit in Indian community. It is a culture in their society where they take it continuously in life and associated with cheek cancer. Users of tobacco either dip, snuff or chewing have a risk of cancer developed over floor of mouth, gum and lip. In our national scenario, oral cancer that affected cheek was closely associated with the habit of betel quid chewing and tobacco snuffing ( Vegers 1979 )
Consumption of alcohol excessively associated with tongue and floor of mouth cancer. The risk even higher for those who drink and smoking. Infection with virus ( Human papilloma virus ) also another factor which can contributed for oral cancer. The oral lining can get infected through oral sex activity with multiple sex partner. Strong family history of cancer also might cause cancer occurred in certain individual.
Clinically, the disease might manifested as nodular lump or an ulcer over oral mucosal lining, which will continuously grow ( fungating out or infiltrating ) or remained unhealed and painless. The disease will keep growing and the patients will started having symptoms like pain on eating, discomfort and come to the stage that it starts to spread to other part of body especially cervical region which manifested as lymphadenopathy.

Cancer of buccal mucosa (Cheek)

Cancer of lateral border of tongue

Cancer of floor of mouth
Management of oral malignancy will start with history taking, thoroughly clinical examination , biopsy and imaging ( CT scan or MRI ( Magnetic Resonance Imaging ) ) which sometimes involving from brain to hip for staging purpose. It will involved multidiscipline team which comprises surgeon, oncologist, dietitian, psychiatrist and dentist.
Generally, the most superior treatment for oral cancer is surgery. This surgery will involve surgery on neck (neck dissection), wide excision of tumour /cancer and in most occasion reconstructions are required. Adjuvant treatments like radiotherapy and chemotherapy might be given for better disease control. In cases, where surgery is not feasible, concurrent chemo-radiotherapy might be given.
References
- Shah JP, Johnson NW, Batsakis JG, Global epidemiology , Oral Cancer 2003.
- WHO Meeting 1984. Control of oral cancer in developing country. Bulletin of World Health Organization .
- Zain RB, Ikeda N, Razak IA, Axell T, Majid ZA, Gupta PC, Yaacob M (1997). A national epidemiology survey of oral mucosal lesions in Malaysia. Community Dentistry.
- Veger JWM.( 1979 ) Squamous cell carcinoma of buccal mucosa : A review of 85 cases. Arch Otolaryngology.
| Last Reviewed | : | 20 March 2015 |
| Writer | : | Dr. Mohd. Nury b. Yusoff |
| Accreditor | : | Dr. Mannil Thomas Abraham |
| Reviewer | : | Dr. Mukhriz bin Hamdan |





