

Introduction
The lungs is an organ containing millions of alveoli which is responsible for the exchange of oxygen and carbon dioxide. Pneumonia is the inflammation or infection in the lungs. This happens when the alveoli are filled up with inflammatory cells. As a result, gas exchange is compromised. Penumonia is usually caused by bacterial infection, virus but sometimes it could be due to fungus and parasites. It can also result from exposure to chemical or physical substances. Symptoms of pneumonia includes cough, chest pain, fever and shortness of breath. Penumonia can be diagnosed from history from the patient, physical findings, chest radiograph and sputum examination. The treatment depends on the cause of the pneumonia; bacterial pneumonia is treated with antibiotics. Pneumonia affects all age groups and is one of the most common cause of death in patients with chronic disease. Vaccines are available for pneumonococcal pneumonia. The prognosis of pneumonia depends of type of pneumonia, complications and co-morbidity conditions in a patient.
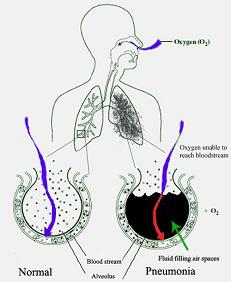
Illustration: Oxygen cannot enter the lungs in pneumonia
Epidemiology
Pneumonia is a common condition worldwide. It is a major cause of death in all age groups and the main cause of death in children in low income countries. The World Health Organization (WHO) predicts that the death is less in adults but is on the rise the elderly.
In the United Kingdom, the rate of pneumonia is 6 cases every 1000 population age range 18-39. For the elderly (age 75 and above), the value increases to 75 cases for every 1000 population. Twenty to 40% patients requires hospital admission and from this out of this, 5-10% are treated in the Incentive Care Unit. Death rate in the United Kingdom is 5-10%.
Classifications of Pneumonia
Community Acquired Pneumonia
This is the most common type of pneumonia. The causal organism are those that is found in the community. Bacteria organisms are such as Streptococcus pneumoniae, Haemophilus influenza Staphylococcus aureus and atypical organisms such as Moxiella catarrhalis, Chlamydia pneumonia and Legionella penumophilia and Mycoplasma pneumoniae. In Malaysia, Mybacoteruim tuberculosis which causes tuberculosis is one of the most commonest cause of pneumonia in the community. Genrally, Streptococcus pneumonia is the commonest cause of pneumonia worldwide. Viruses that causes pneumonia are influenza virus, respiratory syncitial virus, adenovirus, parainfluenza virus and the H1N1 viruses. Apart from bacteria and viruses, other organisms that can cause pneumonia are parasites such Toxoplasma gondii, Strongyloides stercoralis dan Ascaris. These organism entres the body via the skin or feco-orally and reaches the lung via the blood stream. Parasites can cause an immune reaction which is called “eosniophilic pnuemonitis”.

Illustration of Lung under a microscope : Normal and Pneumonia
Hospital Acquired Pneumonia
Also know as nosocomial pneumonia. This type of pneumonia occurs after 72 in hospital or after 72 or discharge from hospital due to other conditions. Causal organisms are Klebsiella, Pseudomonas, Enterobacter, Serratia and Methicillin Resistant Staphylococcus Aureus (MRSA). Hospital acquired pneumonia is more serious compared to community acquired pneumonia.
Factors which predisposes to hospital acquired pneumonia are prolonged malnutrition, cardiac and lung diseases, and low gastric acid. All these factors reduces the immune system to overcome an infection. Pneumonia associated with ventilation (Ventilator-associated-pneumonia) is a subset of nosocomial pneumonia when it occurs 48 hours after invasive ventilation.
Healthcare associated Pneumonia (HCAP)
This type of pneumonia affects residents of health facilities such as nursing homes.
Pneumonia in the Immunocompromised/Immunosuppressed
These are group of patients such as people living with the human immunodeficiency virus (PLHIV) or those with acquired human immunodeficiency syndrome (HIV), patients receiving chemotherapy or steroids, chronic renal failure patients and cancer patients. Organisms involved are similar the ones above, however they can also be infected by germs which do not cause harm to normal individuals, these are the cytomegaloviruses, Pneumocystis jiroveci, Penumocystis carini, Cryptococcus neoformas, Coccidioides immitis and Histoplasma capsulatum, Mycobacterium avium-intercellulare and ‘invasive aspergillosis or ‘invasive candidiasis’.
Others
-
- Severe acute respiratory syndrome (SARS)
This type of pneumonia is very contagious, dangerous and can cause death. It is due to a corona virus SARS which was first discovered in China in 2002.
- Severe acute respiratory syndrome (SARS)
-
- Chemical Pneumonitis
This type of pneumonia is caused by chemical agents such pesticides which is inhaled.
- Chemical Pneumonitis
-
- Aspiration Pneumonia
This occurs when materials from the mouth or gastric contents are aspirated into the lungs. Apart from aspirating toxic agents anaerobic organisms can also be aspirated. This type of pneumonia is one of the main cause of pneumonia among patients with poor gag reflex for example those who are comatose.
- Aspiration Pneumonia
- Interstitial Pneumonia
This involves the space between one alveolus and another. Usually caused by viruses or atypical bacteria.
Symptoms
The presenting symptoms are cough productive of yellow or green sputum, high grade fever, chills, blood stained sputum or shortness of breath. For Streptococus pneumonia the sputums is typically described as rusty coloured. Some patients experience chest pain during inspiration, which is called pleuritic chest pain. Other constitutional symptoms are loss of appetite, weight loss, headache, sweating, joint and muscle aches. In the elderly there may manifest as confusion.
Signs
Fever (>38 o C) is a common sign. Increased breathing and heart rate to more than 20 per minute and more than 100 per minute respectively. Breathless patients with impaired conscious level should be treated urgently. Chest examination with a stethoscope may reveal abnormality, however some patients may not show any signs.
Systemic Symptoms:
High Grade Fever
Rigors
Headache
Loss of appetite
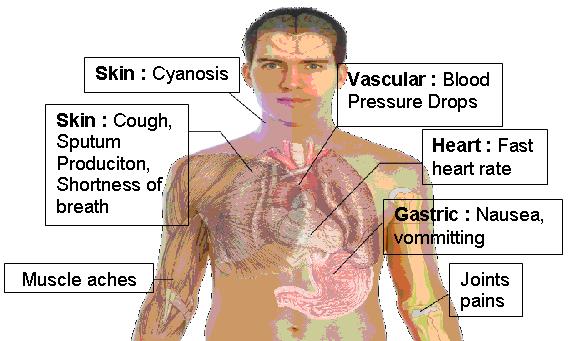
Illustration: Symptoms of Pneumonia
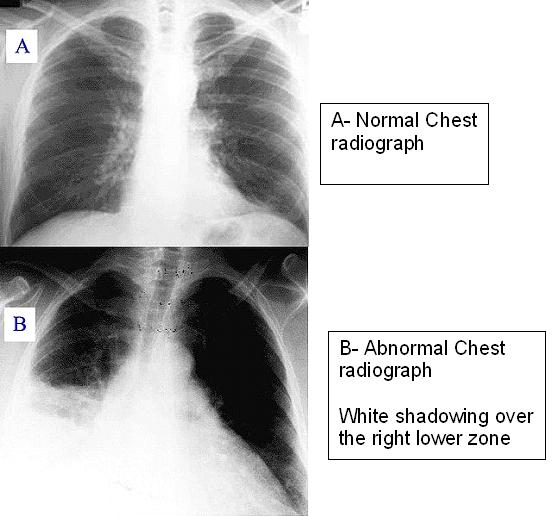
Investigations
Sputum is taken for examination under the microscope, it is also cultured for organisms including for tuberculosis. Chest radiograph to look for signs of pneumonia or it’s complication. Rarely a computerized tomography (CT) done to look for other diseases. Blood is taken to see reaction towards bacterial infection whereby the total white count will be elvevated, however for those who are immunocompromised this can be reduced. Blood cultures and sensitivities for organisms will also be done, and if it positive, this is called bacterima or septicaemia. Serological tests can also be done for Mycoplasma, Legionella, Chlamydia and Legionella. Throat swab is taken for H1N1 testing. Tracheal secretions can be tested for viruses such as influenza, respiratory syncytial virus and adenoviruses. Blood investigations for kidney and liver function is taken to look for complication as a result of septicaemia.
Treatment
Not all patients will be admitted to hospital but treated as outpatients. Antibiotics if given orally, patients is advised to drink lots of fluids and rest. Over the counter cough medicine are not effective for pneumonia. If symptoms does not improve or become worse, patients are advised to come in for admission to hospital. Those who have shortness of breath, immunocompromised and the elderly are usually admitted.
Community acquired pneumonia are treated with antibiotics such as ampicillin or/erythromycin for 7 to 10 days. Hospital acquired pneumonia are treated with cephalosporin, aminoglycosides or carbepenem group of medication which are given intravenously.
Prevention
Cessation of smoking is stressed to patients. Patient with AIDS can be given prophylaxis with an antibiotic. Prophylaxis with pneumococcal vaccine for prevention of Streptococcus pneumonia is useful for patients is chronic lung diseases, diabetics, liver impairment and those whose spleen has been removed. Prophylaxis is given every 5 years.
Prophylaxis with influenza vaccine is advised yearly for adults especially for healthcare workers, residents of nursing homes, asthmatics and pregnant ladies.
References
- Pneumonia at eMedicine Dictionary
- Pneumonia at Dorland’s Medical Dictionary
- Causes of death in neonates and children under five in the world. World Health Organization 2008.
- Kabra SK, Lodha, R Pandey RM 2010. Antibiotics for community acquired pneumonia in children. Cochrane Database Syst. Rev. 3: CD004874
- Hoare Z, Lim WS 2006. Pneumonia: update on diagnosis and management. BMJ 332 (7549).: 1077-9
- Table 13-7 in: Mitchell, Richard Sheppard; Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson
- Krause DC Balish MF February 2004. Cellular engineering in a minimal microbe: structure and assembly of the terminal organelle of Mycoplasma pneumonia. Mol. Microbiol. 51 (4): 917-24
- Anevlavis S, Bouros D February 2010. Community acquired bacterial pneumonia. Expert Opin Pharmacother 11 (3): 361-74
- Figueiredo LT September 2009. Viral Pneumonia: epidemiological, clinical, pathophysiological and therapeutic aspects. J Bras Pneumol 35 (9): 899-906
- Metlay JP, Kapoor WN, Fine MJ November 1997. Does this patient have community-acquired pneumonia? Diagnosing pneumonia by history and physical examination. JAMA 278 (17): 1440-5
- Wipf JE, Lipsky BA, Hirschmann JV et al. May 1999. Diagnosing pneumonia by physical examination: relevant or relic?. Arch. Intern. Med. 159 (10): 1082-7
- Heckerling PS, Tape TG, Wigton RS et al (1990). Clinical prediction rule for pulmonary infiltrates. Ann. Intern. Med. 113 (9): 664-70
- Emerman CL, Dawson N, Speroff T et al. Comparison of physician judgement and decisions for ordering chest radiographs for pneumonia in outpatients. Annals of emergency medicine 20 (11): 1215-9
- Syrjala H, Broas M, Suramo I et al. High resolution computed tomography for the diagnosis of community-acquired pneumonia. Clin. Infect. Dis. 27 (2): 358-63
- ChangCC, Cheng AC, Chang AB (2007). Over the counter (OTC) medications to reduce cough as an adjunct to antibiotics for acute pneumonia in children and adults. Cochrane Database Syst Rev 4
- Scalera NM File TM. How long should we treat community acquired pneumonia?. Curr. Opin. Infect. Dis. 20 (2): 177-81
- Guidelines for the management of adults with hospital-acquired, ventilator-associated and healthcare associated pneumonia. Am J Respir Cri Care Med 171 (4): 388-416
- WHO (1999). Pneumococcal vaccines. WHO position paper. Wkly. Epidemiol. Rec. 74 (23): 177-83
| Last Reviewed | : | 5 August 2013 |
| Writer | : | Dr. Norhaya Mohd Razali |





