

Squint or strabismus refers to a misalignment of the eyes. It is also known as crossed eyes, characterized by eyes that do not look towards an object together. Eyes may cross, or one may look in another direction. This may occur all the time or only during certain period example during stressful times. Crossed eyes may occur in newborns (congenital strabismus) or later in life, which can cause problems with double vision. There are many different types of squint, but broadly they can be divided into the following groups:
- Esotropias
An esotropia is the medical name for a convergent squint where one eye turns in towards the nose.

- Exotropias
An exotropia is the medical name for a divergent squint where the one eye turns outwards.

- Hypertropias and Hypotropias
These terms refer to vertical squints where one eye is higher (hypertropia) or lower (hypotropia) than the fellow eye.

- Paralytic Squints
There are three nerves which send signals to the six eye muscles, these are the third, fourth and sixth cranial nerves. Damage to these nerves as result of poor blood supply to the nerve, pressure on the nerve or head injuries will cause limited eye movements and paralytic quint
Squint surgery (also known as extraocular muscle surgery, eye muscle surgery, or eye alignment surgery) is surgery on the external muscles of the eye (extraocular muscles) to correct the misalignment of the eyes.
Eye muscle surgery does not fix the poor vision of a lazy eye. A child may have to wear glasses after surgery. In general, the younger a child is when the surgery is done, the better will be the result.
Adults with mild strabismus that comes and goes may do well with glasses and eye muscle exercises to help keep the eyes straight. More severe forms of adult strabismus will need surgery to straighten the eyes. If strabismus has occurred because of vision loss, the vision loss will need to be corrected before strabismus surgery can be successful.
Strabismus surgery can be done as daycare or in-patient surgery. The average duration of the surgery is variable. After surgery, the patient should expect soreness and redness of the operated eye. In cases of re-operations, more pain is expected. It also leaves redness that lasts longer and may cause some vomiting in the early post-operative period.
Types of squint surgery include:
- Loosening / weakening procedure
- Tightening / strengthening procedure
- Transposition / repositioning procedure
- Adjustable suture surgery is a method of reattaching an extraocular muscle by means of a stitch that can be shortened or lengthened within the first post-operative day, to obtain better ocular alignment.
Indication
The indications for strabismus surgery vary depending on the age and the particular needs of the patient.
The primary indications for strabismus surgery are:
- Double vision
- Reduced or threatened binocularity
- An abnormal head position secondary to eye misalignment
- A constricted visual field secondary to squint
- Poor cosmetics secondary to eye misalignment.
Contraindication
Surgery should not be performed to correct congenital strabismus when the patient has a life-limiting condition or a medical condition that precludes the safe administration of anaesthesia. Surgery should be delayed when the accomodative component has not been treated or when measurements of squint (eg. degrees of misalignment) are unstable
Pre-op evaluation
Before surgical correction can be recommended, an attempt should be made to correct the deviation with non-surgical methods such as spectacles. Visual acuity should be equalized by treating amblyopia, any accommodative component should be treated with spectacles. Good and equal visual acuity will help to stabilize the ocular alignment once surgery has been performed.
Size of deviation
Surgical correction is recommended when esotropia is greater than 15 prism diopters. Esodeviations of less than 15 prism diopters are not considered large enough to impede the development of fusion and not unsightly enough to require surgical correction.
Timing of the operation
Timing of surgical correction for strabismus varies according to cause. Surgical correction of infantile esotropia generally is not recommended until the size of deviation is stable on repeated examinations. Study showed that children with this problem have a better chance of developing fusion and binocularity when they undergo surgery before the age of 2. Patients with esotropia related to a sixth-nerve palsy are usually observed for 6 months before surgery is recommended because recovery of lateral rectus function may occur during this period.
Complications
Fortunately, serious complications following squint surgery are rare. These include:
- Slipped muscles
A slipped muscle occurs when the stitches holding the eye muscle to the outer coat of the eyeball break or loosen and the muscle moves backwards to a position behind the eyeball. This rare complication (approximately 1 in 400 cases) can occur during, or in the first week after the operation. If it occurs after the operation the patient / parents will notice that the eye position has suddenly changed and that they / their child cannot move the eye in one particular direction. They may also be aware of double vision. Further surgery to find the slipped muscle and stitch it securely to the sclera is required within 24 hours. Very occasionally it is not possible to find the slipped muscle (this is then called a lost muscle) and a different type of operation is needed to try and improve the alignment of the eyes. - Scleral (white part of eye) perforation ?
This refers to the penetration of the outer coat of the eyeball with a surgical needle. The incidence of this complication is thought to be in the region of 1-2% of cases. Scleral perforations in children often require no treatment. A scleral perforation in an adult is usually treated by applying a “freezing” probe to the site of the perforation, to minimise the risk of developing retinal detachment. A course of antibiotics may also be prescribed to minimize the risk of infection developing in the eye./li> - Infection
The risk of infection developing in the eye (endophthalmitis), which could permanently damage the vision in the eye, is 1 in 20,000 cases. - Surgically Induced Necrotising Scleritis (SINS)
A rare complication of squint surgery in adults that results in marked inflammation of the sclera. Treatment with steroid tablets and other immunosuppressant medication is needed to control this inflammation. - Minor complications following squint surgery include:
- Conjunctivitis which is usually short lived and improves with a course of antibiotic drops.
- A suture granuloma is an area of inflammation around one of the stitches in the eye muscles, before the stich dissolved completely. A short course of steroid drops will usually settle this down.
Outcome
Surgical intervention can result in the eyes being entirely aligned (orthophoria) or nearly so, or it can result in an over- or under correction that may necessitate further treatment or another surgical intervention. The likelihood that the eyes will stay aligned over the longer term is higher if the patient is able to achieve some degree of binocular vision (both eye perceive image of same object simultaneously) after surgery.
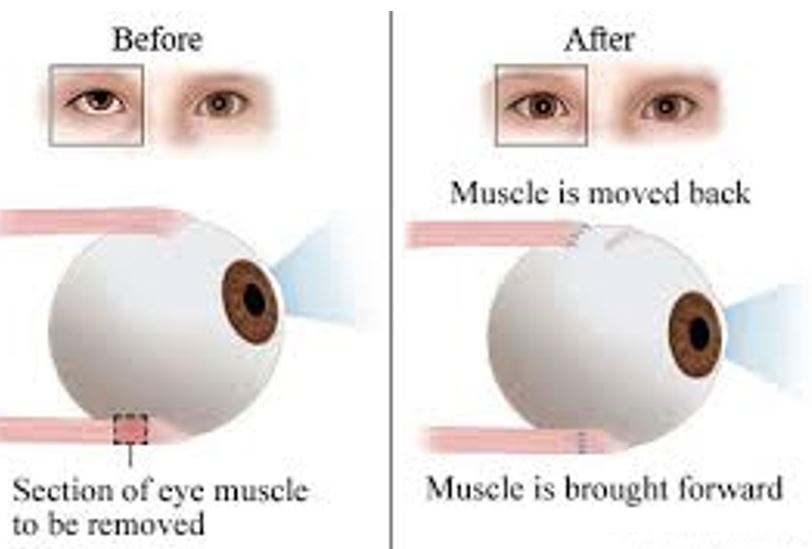
Diagram showing squint before and after surgery
Reference
- www.rch.org.au/ophthal/patient_information/About_Squint_Surgery/
- www.nhs.uk/Conditions/Squint/Pages/Surgery.aspx
- www.uhs.nhs.uk/Media/…/Squintsurgeryforadults-patientinformation.pdf
- www.ouh.nhs.uk/patient-guide/…/files%5C100322squintsurgeryadult.pdf
| Last reviewed | : | 23 August 2019 |
| Writer/Translator | : | Dr. Rosniza bt. Ab. Razak |
| Accreditor | : | Dr. Salmah bt. Othman |
| Reviewer | : | Dr. Rosniza bt. Ab. Razak |





