

Stridor is a prominent continuous monophonic sound produced especially during inspiration breathing. It indicates upper airway narrowing which can be due to many causes. (Figure 1)
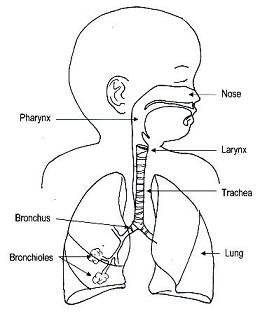
Figure 1: Illustration of children’s airway
Airway narrowing in children causes significant problem because their airway is generally smaller than adult. Any further narrowing will cause significant signs and symptoms. (Figure 2)
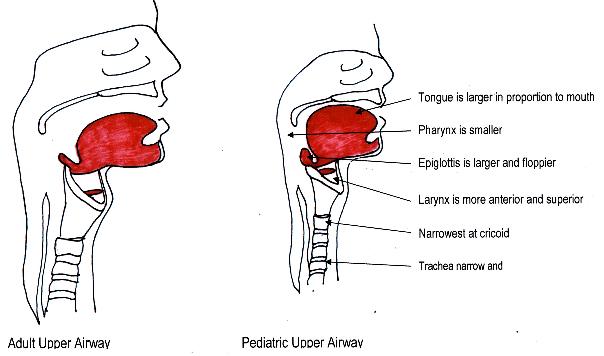
Figure 2: Illustration of children’s airway compared to adult’s airway
Stridor may present as an acute (short term) or chronic (persistent) problem. There are many causes of stridor in children depending on age and presentation. (Table 1)
Causes
|
Acute stridor
|
Persistent stridor
|
|
Table 1: Common causes of stridor in children
|
|
|---|---|
Croup: (laryngotracheobronchitis)
Infection of the upper airway mainly larynx, trachea and bronchus causing airway edema and narrowing
Laryngomalacia:
Congenital condition in young infant due to weakness of the larynx i.e. epiglottis causing collapse or narrowing of the airway (Figure 3).
Subglottic stenosis:
Stenosis or narrowing of the airway at the level of subglotits (below the vocal cord). The underlying causes can be due to congenital or acquired. Commonest cause of acquired subglottic stenosis is post endotracheal intubation injury
Tracheomalacia:
Narrowing at any level of the trachea due to congenital weakness of the airway cartilage. Condition may improve with age but severe tracheomalacia can caused death. (Figure 4)
External compression:
Compression from any structure or lesion from outside the airway can cause stridor. e.g. tumor, abscess, lymph node, abnormal blood vessels etc.
Haemangioma;
Growth from the blood vessels in or near the airway can cause airway obstruction. Severity of airway narrowing depends on the size and site of the haemangioma.
Foreign body inhalation:
Any form of foreign body inhalation that block the airway partially caused stridor. E.g. of foreign body, peanuts, toys, hairclip etc Complete obstruction of the large airway lead to death.
Laryngreal cysts
Arise from blockage of submucosal gland or obstruction of the laryngeal saccule. Symptoms depend on varying degree of obstruction.
Vocal cord paralysis
Reduce or absent of movement of both vocal cords. May be due to injury folloing intubation or injury to laryngeal nerve following surgery, underlying neurological disorders or idoipathic.
|
|
|
|
|
Figure 3: Bronchoscopy findings of: |
||
|
|
|
|
|
Figure 3: Bronchoscopy findings of: |






Signs and Symptoms
Stridor can be accompanied by other symptoms such as difficulty in breathing, coughing, fever, difficulty in feeding and impaired growth.
Other features that may support the diagnosis are like presence of skin haemangioma, abnormal cardiac sounds (Murmur), history of choking prior to the onset of symptoms, history of endotracheal intubation, worsening symptoms with respiratory tract infection etc.
Complications
Severe and significant stridor in children causes several complications like recurrent pneumonia, growth retardation, breathing difficulty, bluish discoloration (cyanosis) and interrupted feeding.
Treatment
Treatment depends on the underlying causes.
Mild to moderate laryngomalacia, tracheal stenosis, tracheomalacia, subglottic stenosis may not require specific treatment. However some moderate to severe conditions require intervention either surgical or non-surgical.
Any foreign body inhalation required removal urgently and must be done by a competent surgeon.
Haemangioma management depends on the exact site of the lesion. Medical therapy like steroid and propanolol are indicated. Tracheostomy (Hole in the trachea) to assist the breathing in moderate to severe airway obstruction.
External compression treatment varies with the underlying aetiology e.g. specific tumor treatment, surgery for abnormal blood vessels or medical treatment for infectious causes like Tuberculosis. Laryngeal cysts require surgical removal.
Vocal cord paralysis may require tracheostomy if respiratory symptoms are moderate to severe.
Other supportive treatments which should not be forgotten are good nutritional support and maintaining good oxygenation
Prevention
Congenital (Condition that occur from birth) causes may not have specific preventive measures.
However, prevention of foreign body inhalation in children by close supervision by the adults is useful, immunization to control or reduce the risk of infection and careful endotracheal intubation to prevent airway injury.
Recognizing early sign of stridor followed by early medical consultation is important to prevent complications.
Commonest cause of acute stridor in young baby is viral croup and persistent stridor in baby is laryngomalacia.
| Last Reviewed | : | 02 Mac 2011 |
| Content Writer | : | Dr Asiah Kassim |





