

Introduction
Swallowing problems can affect the quality of life for stroke patients and high risk for lung infection problem. It can be life-threatening if not treated properly. Handling problems of swallowing should aim to make it easier for stroke patients to swallow food safely.
Swallowing problems or dysphagia is a common problem in patients, especially individuals who have suffered from a stroke. It occurs when part of the brain that functions to control the swallowing is damaged or disturbed.
Research shows the incidence rate of swallowing problems reported between 29-67 % in patients with stroke (Martino et al. , 2005, Singh and Hamdy , 2006) and about 15 % of whom were aged over 60 years ( Brady 2008).
Process of Swallowing
Process of swallowing is divided into 4 stages (Hedge 2001, Marks & Rainbow 2003, Logemann 1984), namely:
-
The first stage: Preparation of Bolus Process
The process of chewing food requires closure of the lips to prevent food from going off when chewing. Teeth and jaws help to break food into small pieces and tongue moves the food to the left and to the right to be chewed and softened with saliva to form the bolus. The tongue then moves the bolus toward the back of the mouth.
- The second stage: Bolus Delivery Process
Food / liquid that have become bolus are pushed by the tongue to the back of the mouth until the signal for swallowing triggers from the brain.
-
The third stage: Pharyngeal Phase
It’s a non-voluntarily process. After swallowing signal is triggered, the soft palate is lifted so that the bolus of food / fluid is allowed into the pharynx and avoids the food goes into the nose. Throat will move upwards and forwards to allow the respiratory tract closed and the food passage opened. Bolus will fall from the mouth into the throat and progresses into the esophagus (food passage). All of these processes occur in sequence but very fast (less than one second).
-
The fourth stage: Bolus Delivery from the Esophagus to the Stomach
The esophagus is the muscular tube that connects the throat and stomach and the process coordinated by muscle contractions to push the bolus into the stomach. The esophagus has two valves which top and bottom valve. Both the valves will open to allow the bolus enters the stomach.
Causes of Swallowing Problems Stroke Patients
Swallowing problems are caused by:
-
Cognitive problems – stroke patients is associated with an increased incidence of dementia.
-
Damage to the nerves involved in swallowing.
-
Damage to the brain that control the process of swallowing.
The Effects Swallowing Problems
Swallowing problems if not treated immediately can cause patients to malnutrition, sudden loss of weight, dehydration and infections of the lungs, which can threaten the lives of patients (Smithard et al. 1996).
Signs of Swallowing Problems
Stroke patients who have problems swallowing will show signs such as :
- Drooling at weaker side of the face
- Lack of appetite
- The food remains in the mouth after swallowing
- Difficult / slow to swallow
- Swallow several times for a small bolus
- Choking / cough before / during / after swallowing
- Frequent clear his throat after swallowing
- Fatigue during / after meals
- Takes a long time to chew / eat
- Voice changes to wetness after eating or drinking
- Sudden loss of weight
- Frequent lung infections
Assessment of Swallowing Difficulties
Stroke patients who have difficulty in swallowing should undergo an assessment to be carried out by a Speech-Language Therapist. The assessments are:
-
Clinical Bedside Swallowing Assessment.
The first phase is to identify the functions and structures of the speech organs, signs of swallowing problems and suitability for evaluation using instrumentation such as VFSS or FEES.
- Assessment using An Instrumentation
- Videofluoroscopy Swallowing Study (VFSS)

Source: Speech-Language Therapy Unit, Hospital Kuala Lumpur -
VFSS is a standard assessment through a dynamic x – ray scanning.
-
The assessment is conducted jointly with Radiologist and Radiographer. Radiographer will take moving images captured from a side view. Patients will be given food and drink that was mixed with barium powder to reveal the food movement during the x-ray scanning.
- The assessment is carried out to determine food concentration, swallowing technique and body position appropriate for the patient to swallow safely. VFSS takes 10-15 minutes.
-
- Fibreoptic Endoscopic Evaluation of Swallowing (FEES).
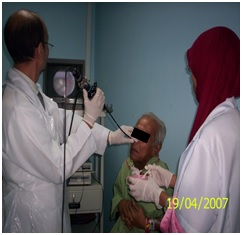
Source: Speech-Language Therapy Unit, Hospital Kuala Lumpur -
FEES is conducted by inserting a flexible endoscope into the nostrils to see swallowing process in the throat. This assessment is simple and safe and can be performed on patients who sit on the bed.
-
It is not exposed to radiation. It allows assessment of anatomy and sensory.
-
- Videofluoroscopy Swallowing Study (VFSS)
Treatment of Swallowing Difficulties
There is no medicine for the problems of swallowing. Swallowing problems can be recovered in several ways, namely:
- Compensatory strategies: Patient is given techniques to swallow safely
- Rehabilitation: Patient is given exercises to strengthen muscles to swallow.
- Airway Protection Techniques: The patient is taught techniques to avoid food enters the airway during eating.
Strategy given will vary from patient to patient by depending on swallowing problems they have.
The main goal of treatment for swallowing problems is to reduce any risk during swallowing and the risk of death associated with lung infections. In addition, the treatment given to patients is to regain a normal diet intake. This in turn can improve the quality of their lives (Singh & Hamdy, 2006).
Get help from a Speech-Language Therapist to manage your swallowing problems.
References
- Martino, R., Foley, N., & Bhogal, S. (2005). Dysphagia after Stroke: Incidence, Diagnosis, and Pulmonary Complications. Stroke, 36, 2756-2763.
- Singh, S. & Hamdy, S. (2006). Dysphagia in Stroke Patients. Postgrad. Medical Journal, 82, 383–391.
- Brady, A. Managing the Patient with Dysphagia. Home Healthcare Nurse, 26 (1): 41–6.
- Lizzy Marks & Deirdre Rainbow (2003). A Speechmark Practical Therapy Manual: Working with Dysphagia. Speechmark.
- Smithard, D.G., O’Neill, P.A., Park, C.L., & Morris, J. (1996). Complications and Outcome After Acute Stroke: Does Dysphagia Matter? Stroke, 27, 1200-1204.
| Last Reviewed | : | 28 August 2020 |
| Writer / Translator | : | Mohd Azmarul bin A Aziz |
| Accreditor | : | Fairus bt. Mukhtar |
| Reviewer | : | Nadwah bt. Onwi |





