

Introduction
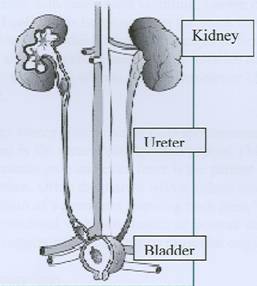
Urine formed in the kidneys flow through tubular structures called ureters into the bladder before being expelled. Urinary stones or calculi can be found anywhere in the kidneys, ureter or bladder. In Malaysia they are commonly found in the upper urinary tract (kidney and ureter). The prevalence of urinary stones in Asia is about 10% – 20% as compared to 15% – 18% in Western countries.
Stones in the urinary tract
A stone forms when a very high concentration or “super saturation” of a certain constituent in the urine causes crystallization. Normally urine contains substances called inhibitors which prevent formation of stones but they may not work in certain cases. This high concentration of urine constituents often occur in people who are regularly dehydrated due to lack of fluid intake. Some patients may have a higher than normal level of these substances in the blood and /or eliminate an increased amount in the urine.Recurrent urinary infection also promotes the formation of stones. When obstruction of the urinary tract occurs e.g an enlarged prostate obstructing the bladder, the stagnation of urine causes recurrent infections and stone formation. Some patients may be born with abnormalities of their urinary tract causing obstruction.
The different types of stones include calcium oxalate, uric acid and cystine stones. Struvite stones are composed of magnesium, ammonium, phosphate, mixed with carbonate. They are commonly known as infective stones. In Malaysia calcium oxalate, uric asid andinfective stones are common.
Signs & symptoms
Kidneys stones often do not cause any pain and may be discovered by chance in an ultrasound or x-ray of the abdomen done for other reasons. Small stones may pass painlessly or cause severe abdominal pain from the back to the groin with nausea and vomiting, known commonly as a renal colic. This happens when the stone travels down the narrow ureter which contracts to expel it. Some patients may also feel a sharp pain in their testicles or along their penis when they urinate. They often notice blood in the urine.
Larger stones which cannot pass spontaneously may get lodged in the ureter causing obstruction. This leads to continuous pain and even fever if the patient develops an infection. Often the patient with a kidney stone may complain of a persistent gnawing back pain. This pain is not associated with movements or posture changes which may suggest pain of a bony or muscular origin.
Investigations
90% of urinary stones can be seen on anx-ray of the abdomen. This is usually followed by a series of special x-rays taken after a dye material in injected into the body, what is known as an intravenous pyelogram (IVP) to see the level of the stone and the presence of any obstruction. An ultrasound is done if a stone is suspected but not seen on the x-ray. This is common of uric acid stones. A more accurate investigation today will be anon contrasted CT-scan of the abdomen where no dye is given but this is only available in bigger hospitals.
A series of blood tests is performed to assess kidney function, calcium and uric acid levels. Urine tests are performed to look for infection, acidity or alkalinity. In certain cases, it is checked for elevated levels of calcium, oxalate or uric acid.
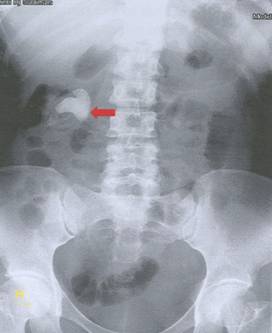
X-ray of the abdomen showing a large right kidney stone

IVP of the same patient showing obstruction by the kidney stone
Complications
A stone in the kidney or ureter may cause obstruction. This leads to infection of the kidneys and in severe cases, pus formation. In turn this infection can spread into the bloodstream and the patient becomes very ill suffering from urosepsis. This condition is an emergency and patient needs treatment with antibiotics and the obstruction relieved by insertion of a tube in the ureter to bypass it or insertion of a tube into the kidney to drain the infected urine. Long standing obstruction leads to damage of the affected kidney and if it happens in both kidneys, the patient may develop kidney failure. Presence of a kidney stone which is not obstructing can also cause repeated infection called pyelonephritis.
Likewise stones in the bladder can also cause infection. This stone may obstruct by being impacted at the bladder neck whereby the bladder joins the urethra, the tube along the penis or in the urethra itself. In this situation, the patient develops retention of urine. In long standing obstruction, the backpressure may affect the ureters and kidney causing kidney failure. The bladder muscle which is unable to overcome the obstruction becomes stretched and develops muscle failure. The importance of this is that the patient may not be able to empty his bladder well even after removal of the stone.
In very rare cases, the longstanding bladder stone may irritate the inner surface of the bladder and causes a cancerous change.
Treatment
Most stones less than 4mm will pass out spontaneously. However patients need surgical treatment if the stone does not pass after a period of observation and continues to cause pain. The stone may grow larger or cause complications e.g. obstruction, infection. Sometimes a stone may not be painful but causes deterioration of kidney function. The treatment of stones depend on the site, size and nature of stones.
Extracorporeal Shockwave Lithotripsy (ESWL)
This is very common procedure whereby the patient lies on a special table and shockwaves produced by a machine penetrates his body and fragment the stone into smaller pieces. The patient then passes out these fragments when he urinates. X-ray or ultrasound is used to locate the stone. This procedure is suitable for kidney stones but not larger than 2 cm and most stones in the ureter that can be seen on x-ray.
It is an outpatient procedure and the patient is usually given injections for analgesia and sedation. Larger stones need several courses of treatment.
Local bruising may occur at the back. Although blood in the urine is usually noted after treatment, occasionally bleeding may cause large clot formation around or within the kidney. If very large this may compress the kidney. Infection may occur and the patient develops fever and back pain. Stone fragments may not pass completely and form a column which obstructs the ureter. For this reason a tube to drain urine from the kidney to the bladder is sometimes inserted before ESWL.

Patient undergoing ESWL
Percutaneous Nephrolithotomy (PCNL)
A procedure whereby the doctor makes a small incision on the patient’s back overlying the kidney area to create a tract that allows insertion of a special instrument with a telescope. The stone is visualized and fragmented using power sources e.g. laser, ultrasonic or pneumatic. At the end of the procedure the patient has a temporary tube draining his kidney. This procedure, performed under general anesthesia, is suitable for stones >2cm as well as kidney stones which have failed ESWL.
Common complications include infection and bleeding during or after the procedure. Sometimes it is not possible to completely clear all the stones and the patient may need another minor procedure through the same incision to remove residual stones.
Ureteroscopy
Ureteroscopy involves passing an instrument through the urethra, bladder and into the ureter. The stone is then fragmented, removed and a temporary tube is placed within the ureter to drain the kidney. It’s a procedure done under anesthesia and is suitable for stones in the ureter which are large, not seen on normal x-rays or fail to fragment at ESWL. Common complications include injury to the ureter, infection and bleeding.
Open surgery
It is rarely performed today because most stones can be removed by less invasive methods. In patients with very big stones in the kidney or ureter it remains an option. Sometimes when a kidney with stones becomes scarred and poorly functioning because of repeated infections, it is removed. There is still a role for open surgery to remove large bladder stones.
Prevention
Once a patient has a kidney stone, he is at risk to form stones again. Patients are advised to drink at least 2-3 litres f fluids a day to keep themselves well hydrated and to dilute their urine. A good guide that one drinks enough is when the urine passed is almost colourless like water. The advice is even more important in our hot climate.
Dietary changes may be required to prevent stone formation. A diet very high in protein may increase elimination of calcium oxalate and uric acid in the urine. Patients who form uric acid stones are advised to reduce purine-rich food e.g. meat, seafood, alcohol. There is no restriction on calcium-rich dairy products to prevent calcium stones; however patients should not consume excessive amounts. Food such as chocolate, coffee, spinach is rich in oxalate and should be consumed in smaller amounts among those who have repeated formation of oxalate-containing stones. In certain conditions patients may have to take medications to prevent the formation of calcium and uric acid stones in the urine. The drug allopurinol may be useful in those continue to form uric acid stones despite dietary measures. This is often combined with a medication to reduce the acidity of the urine.
Support
- Malaysian Urological Association (MUA)
- www.urology-malaysia.org
- National Institute of Diabetes and Digestive and Kidney Disease.
- www.kidney.niddk.nih.gov
| Last Reviewed | : | 27 April 2012 |
| Writer | : | Dr. Susan Woo |
| Reviewer | : | Dr. Sunita a/p Bavanandan |





