

Nearly 1.8% of young adults and 30% of elderly individuals in the population have dizziness (Sloan et al. 2001). Vertigo, a spinning sensation, is usually associated with problems in the vestibular and balance organs.
The vestibular and balance organs in the inner ear are consisted of semicircular canals and otolithic organs which are the saccule and utricle. The vestibular organs will transmit signals to brain via nerves which send signals to body muscles or eyes. When vestibular systems are interrupted, abnormal nystagmus and vertigo could occur. Nystagmus is described as involuntary or jerky movement of the eyes.
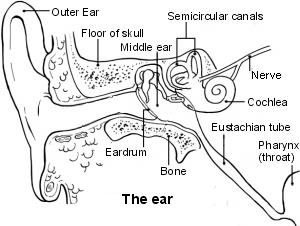 |
| Source: http://www.patient.co.uk/health/Benign-Paroxysmal Positional-Vertigo.htm |
The vestibular and balance tests are performed to evaluate the function of balance organs, the location of lesions in the vestibular organs and associated hearing loss, if any. The problems in vestibular and balance organs can be caused by any pathology in the peripheral or central vestibular systems. The peripheral vestibular problems include Meniere’s Disease, Benign Positionals Paroxysmal Vertigo (BPPV), Vestibular Neuritis and so on. Vertigo caused by the central vestibular problems could be due to the tumor in the hearing nerve, pathology in the cerebellar, Multiple Sclerosis and others. The central vestibular and balance lesions usually involve the nerves or central nervous system and are quite rare.
Patients who are required for vestibular and balance assessments will be referred by the Ear, Nose and Throat doctors or by an audiologists. Besides vestibular assessments, full medical examinations such as blood tests or Magnetic Resonance Imaging (MRI) can be done by doctors to investigate the cause of vertigo (Devesahayam & Narayanan, 2011). The objective of the vestibular and balance assessments is to identify the causes of vertigo therefore medical management or vestibular rehabilitation to improve the patients’ quality of life can be suggested.
Types of Balance and Vestibular Assessments
The audiological assessments for patients with balance and vestibular problems include:
- Hearing tests including otoscopy, tympanometry and pure-tone audiometry
- Electrophysiological tests such as Auditory Brainstem Response (ABR) and Otoacoustic Emissions (OAE)
- The tests of eye movements including gaze, spontaneous nystagmus, saccades, pursuits or optokinetics
- Dix Hallpike
- Caloric testing
- Rotational chair
- Vestibular Evoked Myogenic Potentials (VEMPs)
How We Perform the Tests
Patients will be advised to avoid medications that can suppress dizziness 48 hours prior to testing.
Before the testing commenced, hearing status will be checked using tympanometry and pure-tone audiometry to determine the level and type of hearing loss. Audiometry is a hearing test that requires patient to press response button to the faintest sound that the patient could hear.
Auditory Brainstem Response is a electrophysiology test that is done to identify retrocochlear lesions. Retrocochlear lesion is a pathology that occurs beyond cochlea, the hearing organ. The lesion is usually at the auditory nerve or brainstem. Electrodes will be attached on the forehead and behind ears using gel paste. Sound stimulus will be presented using insert earphones or headphones. Results in the forms of waves will be analyzed to determine responses to the stimuli.
Eye movements tests such as gaze, pursuits and saccades are usually done using video-nystagmography in which the patient has to wear a special goggle. The patient will be asked to look and track moving targets without moving their head or body. The test is needed to assess the function of balance organs and any lesion of peripheral or central in origin.
To test the horizontal semicircular canals, caloric testing is done by irrigating warm and cold air or water into each patient’s ear. The patient will be wearing a special goggle and the test assesses the strength of nystagmus towards changes in temperature. During testing, patient will be asked to carry out mental alerting task such as counting backwards or recall certain names to keep them alert.
 |
| Caloric Test |
Dix Hallpike Manouvre is performed to investigate Benign Positionals Paroxysmal Vertigo (BPPV). The test is done by turning the patient’s head to one side at a time and lying down with the head extended. BPPV is a condition when otoconia, fragments inside the vestibule are dislodged and moved into the semicircular canals. The condition can cause vertigo due to head and body changing positions.
Rotational Chair assessment is done to investigate whether vestibular problems occur on one or both sides and to observe any vestibular compensation that might have occurred. The test is a rotational chair system that rotates at certain frequencies with the patient using a special goggle to track nystagmus. It is usually done in a dark room.
 |
| Rotational Chair |
Vestibular Evoked Myogenic Potentials is a test used to evaluate the function of otoliths and Inferior Vestibular Nerve. Like Auditory Brainstem Response (ABR), the electrodes will be attached on the lower forehead and the neck region. Sound stimulus will be presented using insert earphones in patient’s ears one at a time and the patient will be asked to turn to one side or raise their head while lying to obtain response when the muscle contracts.
 |
| Vestibular Evoked Myogenic Potentials |
Other tests such as Dynamic Visual Acuity, Head Impulse Test, Head Shake Test and so on will be done when appropriate.
Vestibular and balance problems that are not treated can cause anxiety, depression and difficulty to perform task at work or at home. Certain patients also reported avoiding activities that they used to do before having vertigo. When the assessments have been performed, Epley or Semont Manouvre can be done to treat Benign Paroxysmal Positionals Vertigo (BPPV). Gaze stabilization exercises or other vestibular rehabilitation activities can be performed when diagnosis have been made. In addition, referrals for medical management and physiotherapy can be made when assessments have been done to help patients to manage their vertigo.
References
- Devesahayam, P.R. & Narayanan, P. (2011). Key Concepts in Neurotology. Perak: Hospital Raja Permaisuri Bainun.
- Sloane, P.D., Coeytaux, .RR., Beck, R.S. & Dallara, J. (2001). Dizziness: state of the science Ann Intern Med. 1;134 (9 Pt 2):823-32.
| Last Review | : | 29 January 2014 |
| Writer/translator | : | Sharifah Zainon bt S. Mohd Khan |
| Accreditor | : | Nur Azyani bt. Amri |





